Introduction
Body composition assessment is going through a transition moment. For decades, clinical practice relied on body composition methods that describe the external shape of the body or estimate lean and fat mass based on population models; however, the growing complexity of patients—aging, chronic inflammation, multimorbidity, hydroelectrolytic changes—has highlighted an unavoidable need: to understand not only how much tissue a person has, but in what physiological state that tissue is found.
Today, five great families of body composition methods coexist: anthropometry, 3D scanners, portable ultrasound, multifrequency bioimpedance (mfBIA), and DEXA, each designed to answer different questions. All provide value, but none alone captures cellular dynamics, fluid distribution, or membrane integrity, variables that determine the actual functionality of lean tissue.
In this context, bioimpedance spectroscopy (BIS) emerges not as a replacement for traditional body composition methods, but as the missing physiological piece. Its ability to differentiate intracellular and extracellular compartments, estimate membrane capacitance, and describe cellular status complements existing technologies. This integration allows for a more precise reading of clinical risk and a more informed nutritional intervention.
Anthropometry
Anthropometry constitutes one of the most widespread body composition methods in nutritional and functional assessment due to its low cost, portability, and applicability in diverse clinical, community, and sports environments. Its strength lies in the capacity to generate morphological indicators useful for screening and longitudinal monitoring. However, it presents structural limitations that condition its clinical validity.
- Absolute dependence on the evaluator. Even under standardized ISAK protocols, inter-observer variability in skinfolds and circumferences can exceed 6–8%, particularly in subjects with obesity, atypical fat redistribution, or significant muscle loss (Marfell-Jones et al., 2012).
- The inability to discriminate tissue quality. Anthropometric measurements describe external dimensions but do not allow for differentiating between functional lean mass and edematous lean mass, nor identifying changes in intracellular hydration or cellular membrane integrity, which reduces the method’s sensitivity to detect functional deterioration (Norman et al., 2022).
- Dependence on equations derived from specific populations. Classic models like Durnin & Womersley or Jackson & Pollock were developed in young adults with homogeneous body composition and minimal presence of chronic disease. Their application in older adults, people with sarcopenic obesity, or subjects with hydroelectrolytic alterations introduces systematic bias and reduces the external validity of the method (Heymsfield et al., 1997).
3D Scanners and tissue thickness without physiological characterization
3D body scanners have gained popularity for their ability to generate high-resolution volumetric models, allowing the evaluation of circumferences, symmetries, and body geometry with excellent reproducibility. Their utility lies in the objective quantification of external morphological changes, making them valuable tools for aesthetic, biomechanical, and sports monitoring.
However, their scope is strictly morphometric: they do not estimate muscle mass, fat mass, or internal physiological parameters, and their interpretation does not allow for differentiating between changes in lean tissue, adipose tissue, or body fluids (Liu et al., 2023). In clinical contexts where fluid redistribution or cell mass loss precedes morphological changes, their sensitivity is limited (Norman et al., 2022).
mfBIA: practical and accessible, but dependent on the reference model
Multifrequency bioimpedance (mfBIA) has consolidated itself as one of the most utilized technologies in clinical practice and wellness environments due to its portability, speed, and operational ease. Its operating principle is based on the application of electrical currents at distinct frequencies to estimate the body’s resistance and reactance, from which fat mass and fat-free mass values are derived using predictive equations.
Although mfBIA uses multiple frequencies, its ability to precisely separate intracellular (ICW) and extracellular (ECW) compartments is limited, as the analysis is not based on a complete spectroscopic fitting of the tissue’s electrical behavior, but on equations derived from population patterns. This reduces its sensitivity to detect changes in body cell mass, membrane integrity, or fluid displacement, variables that have demonstrated clinical relevance in nutritional and functional prognosis (Barrea et al., 2020; Norman et al., 2022).
DEXA: solid reference, based on fixed assumptions
Dual-energy X-ray absorptiometry (DEXA) remains the reference method for the regional assessment of lean mass, fat mass, and bone mineral density due to its high reproducibility, precision in compartment discrimination, and methodological robustness in clinical and epidemiological research (Liu et al., 2023).
Its ability to offer segmental analysis makes it a fundamental tool for characterizing tissue distribution patterns, assessing osteometabolic risk, and monitoring interventions in controlled contexts (Liu et al., 2023). The consistency of its measurements and the international standardization of its procedures explain why it continues to be considered the gold standard in body composition.
Notwithstanding its consolidated role as a structural reference, it is important to consider that DEXA presents operational limitations that hinder its systematic use in clinical monitoring. Its high cost, the need for specialized equipment, and accumulated exposure to radiation (although low) restrict its applicability in outpatient, pediatric, or frequent evaluation contexts. These logistical barriers reinforce the need to integrate complementary methods that allow for monitoring functional and cellular changes in a more accessible way, without compromising patient safety or monitoring continuity.
Bioimpedance spectroscopy (BIS): the missing physiological dimension
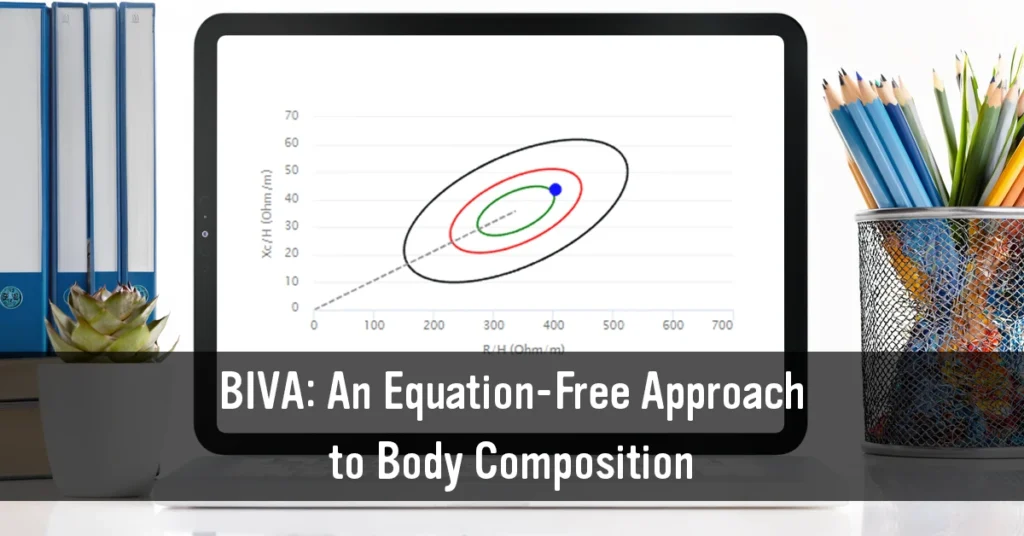
Bioimpedance spectroscopy (BIS), despite being a doubly indirect body composition method to assess body composition, represents a methodological evolution within techniques based on electrical impedance, by modeling biological tissue behavior through the complete fitting of the Cole-Cole plot. This approach allows for the differentiated estimation of extracellular resistance (Re), intracellular resistance (Ri), and membrane capacitance (Cm), variables directly related to fluid distribution and cellular integrity.
Unlike predictive body composition methods based on population equations, BIS characterizes the electrical physiology of the tissue in real time, which makes it possible to quantify intracellular (ICW) and extracellular (ECW) compartments more precisely, as well as detect early alterations in body cell mass, inflammation, or edema, even in the absence of visible changes in weight or circumferences (Bosy-Westphal et al., 2021).
This ability to describe cellular status makes BIS a valuable complement within the ecosystem of body composition methods. Its strength does not lie in substituting consolidated techniques like DEXA, but in providing physiological information that these do not directly evaluate, particularly in scenarios where hydration, inflammation, or fluid redistribution modify the relationship between lean mass, functionality, and clinical prognosis.
Conclusions
Body composition assessment has ceased to be an exercise focused exclusively on the quantification of lean mass and fat mass to become a process that demands integrating morphological, structural, and physiological information. Each of the available technologies brings a distinct perspective on the human body, and their value lies precisely in that complementarity. In contemporary clinical practice, none of the body composition methods alone is sufficient to capture the physiological complexity of patients with inflammation, aging, multimorbidity, or alterations in fluid distribution. The integration of tools that describe structure with those that evaluate physiology allows for a more precise reading of risk, an earlier identification of functional deterioration, and a more informed nutritional intervention.
References
- Barrea, L., Muscogiuri, G., Di Somma, C., Annunziata, G., Megna, M., Falco, A., & Savastano, S. (2020). Phase angle: A biomarker for nutritional status and mortality in hospitalized patients. Clinical Nutrition, 39(9), 2890–2896. https://doi.org/10.1016/j.clnu.2020.01.004
- Bosy‑Westphal, A., Braun, W., & Müller, M. J. (2021). The accuracy of bioelectrical impedance analysis to determine body composition in comparison with dual energy X-ray absorptiometry. Nutrients, 13(2), 357. https://doi.org/10.3390/nu13020357
- Heymsfield, S. B., Wang, Z. M., Baumgartner, R. N., & Ross, R. (1997). Human body composition: Advances in models and methods. Annual Review of Nutrition, 17, 527–558. https://doi.org/10.1146/annurev.nutr.17.1.527
- Liu, T. L., Liu, Y., He, Q., Yang, L., Wang, J., & Li, Y. (2023). Validity of body composition assessment methods in adults: A systematic review and meta-analysis. Obesity Reviews, 24(5), e13557. https://doi.org/10.1111/obr.13557
- Marfell‑Jones, M., Stewart, A., & de Ridder, J. (2012). International standards for anthropometric assessment. International Society for the Advancement of Kinanthropometry (ISAK).
- Measurement. (2025). Limitations of DEXA as a reference method in body composition assessment: A critical appraisal. Measurement, 250, 116809. https://doi.org/10.1016/j.measurement.2025.116809
- Norman, K., Stobäus, N., Pirlich, M., & Bosy‑Westphal, A. (2022). Bioelectrical phase angle and impedance vector analysis—Clinical relevance and applicability of impedance parameters. Clinical Nutrition, 41(4), 1023–1036. https://doi.org/10.1016/j.clnu.2021.12.012
- Piccoli, A. (2004). Bioelectric impedance measurement for fluid status assessment. Seminars in Nephrology, 24(4), 432–437. https://doi.org/10.1016/j.semnephrol.2004.06.009
- Siri, W. E. (1956). Gross composition of the body. In C. A. Tobias & J. H. Lawrence (Eds.), Advances in biological and medical physics (Vol. 4, pp. 239–280). Academic Press.
- Wang, Z. M., Deurenberg, P., Guo, S. S., Pietrobelli, A., Wang, J., Pierson, R. N., & Heymsfield, S. B. (2000). Six-compartment body composition model: Inter-method comparisons of total body fat measurement. International Journal of Obesity, 24(5), 629–639. https://doi.org/10.1038/sj.ijo.0801226