


(The original language of this article is French, and the graphs are shown from actual screenshots in the original language)
Within the organism, the hormonal system is responsible for transmitting messages in the form of hormones that allow the regulation of major physiological functions. One of the main organs of this system is the thyroid, which is responsible for the production of thyroid hormones, called T3 and T4, that play an extremely important role in regulating body metabolism¹. These hormones are particularly responsible for stimulating the breakdown of lipids in the body, lipolysis². Two pathologies can affect this organ: hyperthyroidism, where the thyroid produces an excessive amount of hormones, and hypothyroidism, where the thyroid does not produce enough hormones. Given the role of thyroid hormones, these pathologies will also influence individuals’ body composition.
In this case study, we will focus on the body composition changes induced by nutritional management and physical activity in a patient with hypothyroidism.
| Sex | Male |
| Age | 69 years |
| Height | 169 cm |
| Weight | 99,40 kg |
| BMI | 34,80 kg/m2 |
| Pathologies | Hypothyroidism |
Quick Analysis

First, we can observe that this person has an excess fat mass of 7.42 kg and muscle mass of 8.19 kg, along with slight dehydration with a water deficit of 0.89 L. Considering the patient’s weight and the fact that he is or has been an athlete, his muscle mass is consistent, and we also observe a very high bone mass index, indicating that he has sufficient muscle and bone mass to engage in high-intensity sports activities.

The phase angle, on the other hand, is high considering his age and pathology. However, considering his body mass and level of physical activity, it maintains good cellular quality. It is interesting to note that hypothyroidism does not seem to affect the phase angle.
Fat Mass at Constant Hydration, Total Skeletal Muscle Mass, and Limb Muscle Mass
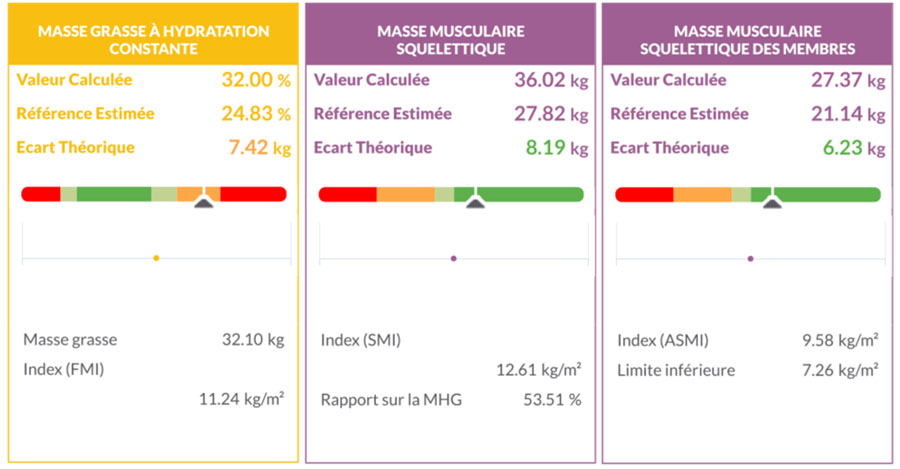
As observed in the quick analysis, this patient has a fat mass 7.42 kg higher than his reference, giving him a fat mass percentage of 32%. The total skeletal muscle mass and limb muscle mass are 36.02 kg and 27.37 kg respectively, which are high when considering the differences with the references. Therefore, he has sufficient muscle mass to engage in high-intensity sports activities, confirmed by the muscle mass/weight ratio of 36.02%, knowing that the lower limit is 31.5% for sarcopenic obesity. If this ratio were below 31.5%, it would mean that this patient’s skeletal muscle mass is insufficient to support his body mass, although his muscle mass is higher than the reference, a characteristic situation of sarcopenic obesity.
Bone Mineral Content, Fat-Free Dry Mass
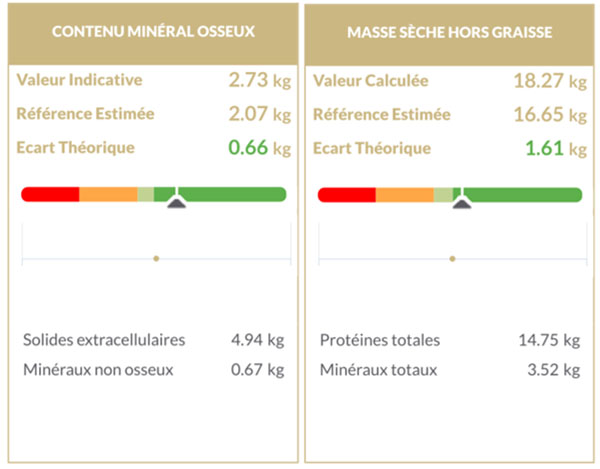
The bone mineral content of this patient is high, with a value of 2.73 kg, 660 g above his reference, confirming the information given by the muscle load and total load indices, indicating that this individual’s bone mass is sufficient to support his body mass without problems. The fat-free dry mass value is 18.27 kg, which is 1.61 kg higher than the reference, confirming that the higher skeletal muscle mass is not only due to good hydration but also to a greater amount of proteins.
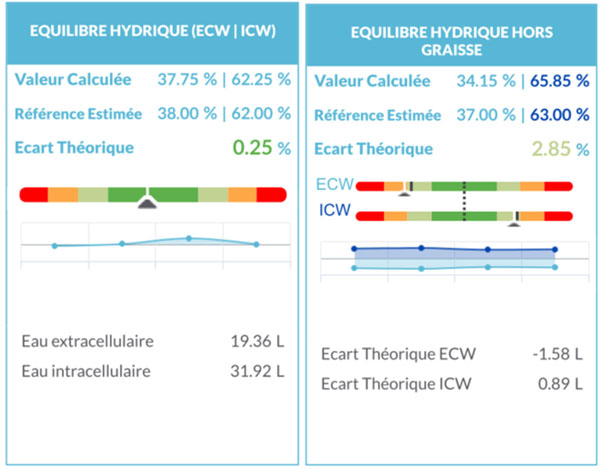
Hydratation
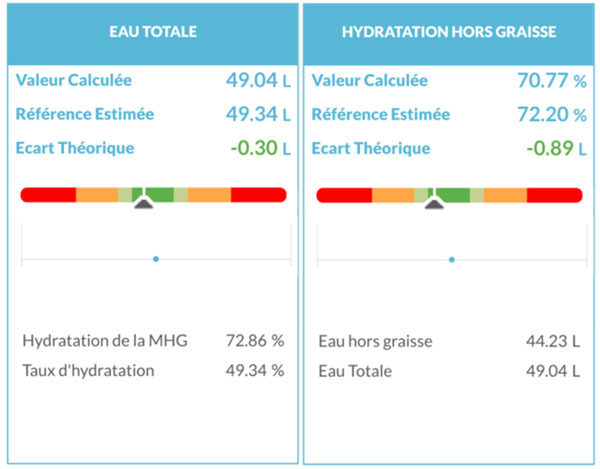
We can observe normal hydration in this patient with a fat-free mass hydration rate of 72.86%, close to the ideal hydration reference value of 73.3%. When looking at fat-free hydration, we see that the theoretical gap between the calculated value and the reference value is -0.89 L, which represents a larger deficit than observed in total water. This difference is explained by the fact that, according to compartment logic, fat mass only includes the lipids of adipose tissue; therefore, the water in adipose tissue is found in the fat-free mass. Thus, the greater the fat mass (and therefore adipose tissue), the more water is added to total water, creating some biases in interpretation. You can find more details on these issues in the dedicated case study at this link. In this patient, this shows that he has slight dehydration at the time of measurement.
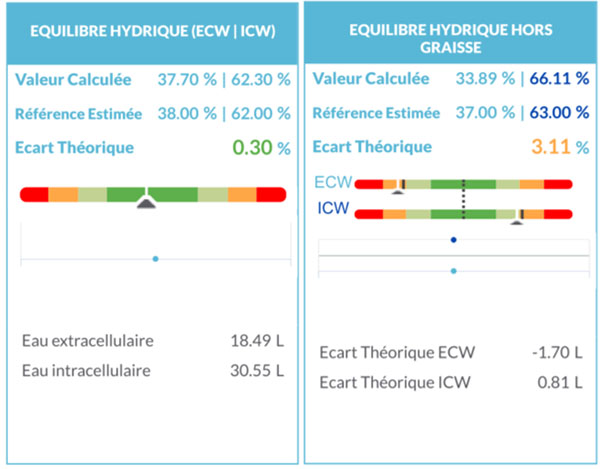
The water balance shows that water would be properly distributed between intra- and extracellular compartments, in addition to being at a normal fat-free mass hydration rate. However, the fat-free water balance indicates that this patient has a significant imbalance in water distribution in the fat-free mass. Indeed, he has significant extracellular dehydration associated with significant intracellular overhydration, with a deficit of 1.70 L and 0.81 L, respectively. This distribution is explained by the specific water distribution of adipose tissue, where 80% of the water is located in the extracellular space; thus, this excess extracellular water can mask, globally, an imbalance in the fat-free mass. In this patient, this translates into a normal global water balance but a significant fat-free imbalance. This distribution could be a consequence of hypothyroidism; however, it seems that this pathology chronically modifies water distribution, so this could be the consequence of slight dehydration and/or treatments for this person.
Quick Analysis – 3 Months After the Start of the Intervention
| Sex | Male |
| Age | 69 years |
| Height | 169 cm |
| Weight | 102,10 kg |
| BMI | 35,75 kg/m2 |
| Pathologies | Hypothyroidism |
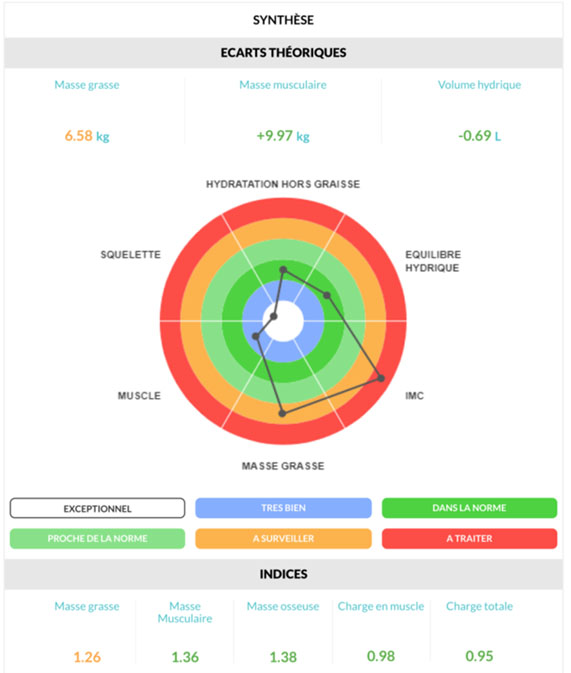
After 3 months of management, we can observe a gain of 2.7 kg with what seems to be a loss of fat mass, a gain in muscle mass, and bone mass as suggested by the theoretical differences and indices. However, in this case, it is relevant not to stop at these differences but to check the values on the corresponding measurements.

We can also observe that the phase angle has not changed between the two measurements, showing that cellular quality has been maintained with the management.
Fat Mass at Constant Hydration, Total Skeletal Muscle Mass, and Limb Muscle Mass
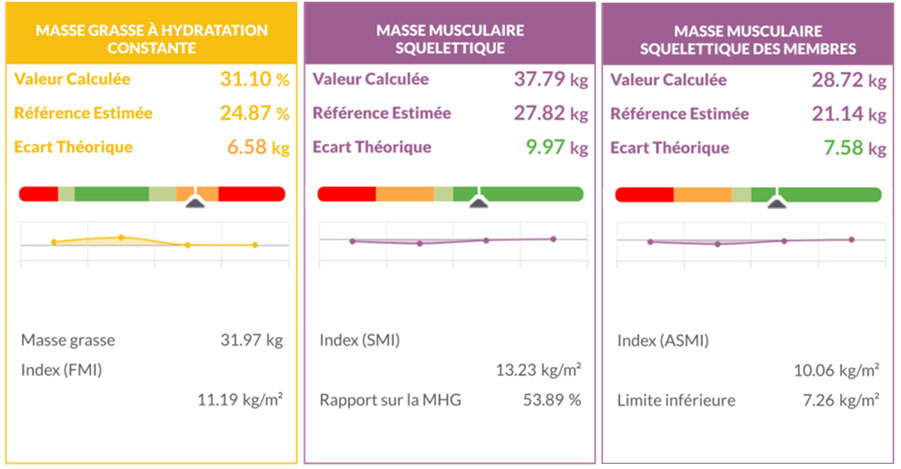
Between the two measurements, we can observe a fat mass loss of 103 grams, resulting in a decrease from 32% to 31.10% fat mass. Given that the fat mass percentage is calculated by dividing the fat mass by the weight, this decrease is mainly due to the weight gain of this patient. For skeletal muscle mass, this patient gained 1.77 kg of total skeletal muscle mass, including 1.35 kg in the limbs, indicating that the weight gain is mainly due to an increase in muscle mass and not fat mass.
The lack of fat mass loss is explained by the hypothyroidism that this person has since thyroid hormones play an important role in stimulating lipolysis. Indeed, thyroid hormones stimulate the mobilization of lipids in adipose tissue and the ability of various organs to use these lipids to produce energy, especially during exercise.
Thus, patients with hypothyroidism use very little lipids to produce energy, making it very difficult for them to lose fat mass.
Bone Mineral Content, Fat-Free Dry Mass

After three months of interventions, the bone mineral content has remained stable, while the fat-free dry mass has increased by 580 g, which is explained by the patient’s physical activity and is consistent with the observed increase in muscle mass. Indeed, about 25-30% of skeletal muscle is composed of contractile proteins, the rest being intramuscular water, and considering both increases, the increase in fat-free dry mass represents about 35% of the increase in skeletal muscle mass.
Hydratation
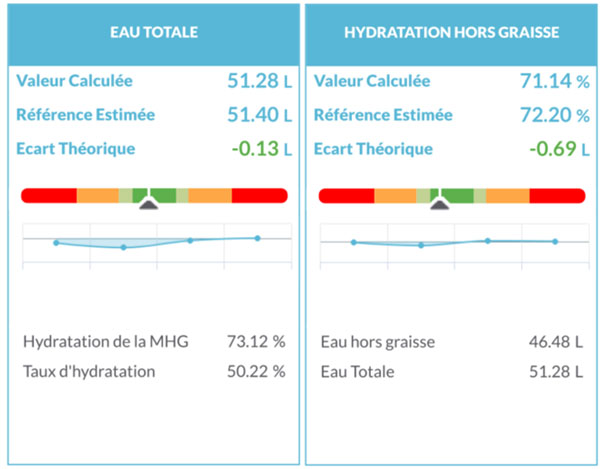
In the same way as in the first measurement, we can observe that this patient has a very good fat-free mass hydration rate (Fat-Free Mass Hydration), confirmed by the “fat-free hydration” measurement of 71.14%.
Regarding water balance, the situation observed in the first measurement is also present for the water balance: the total water balance shows a normal distribution of water between the intra- and extracellular spaces; however, a fat-free mass imbalance remains. Therefore, this alteration in distribution would be a consequence of his pathology and/or treatment and not of an unbalanced lifestyle, as in that case, the return to a balanced lifestyle, created by nutritional management and physical activity, would have corrected this situation.
Conclusion
This case study shows the importance of considering the hormonal status that can be altered by a pathology during fat mass loss, such as hypothyroidism, or by lifestyle (stress, fatigue,…) to optimize it. If the person has a pathology, it is recommended that the patient discuss it with their doctor so that it can be taken into account in their therapy.