(The original language of this article is French, and the graphs are shown from actual screenshots in the original language)
Malnutrition is a condition characterized by a body mass loss greater than 5% in 1 month according to the Haute Autorité de Santé¹, which can be a consequence of a pathology such as cancer² or admission to intensive care³, and whose main consequence is an increase in mortality⁴, ⁵. During their hospitalization, about 40% of Covid-19 patients developed malnutrition⁶, significantly increasing their chances of admission to intensive care and decreasing their survival⁷. The onset of this malnutrition is related both to the pro-inflammatory environment and the loss of taste and smell associated with the pathology⁸, reducing food intake and promoting the loss of body tissue, particularly muscle. Like other pro-inflammatory pathologies, it is therefore necessary to monitor the onset of malnutrition in Covid-19 patients. In this case study, we will focus on a case of malnutrition in a patient with Covid-19 and on the parameters that can be used to detect and/or monitor the evolution of this malnutrition.
| Sex | Female |
| Age | 67 ans |
| Height | 165 cm |
| Weight | 58 kg |
| BMI | 21,3 kg/m2 |
| Pathologies | Covid-19 |
| Symptoms | Asthenia, respiratory difficulties, fever, loss of appetite, and changes in taste and smell |

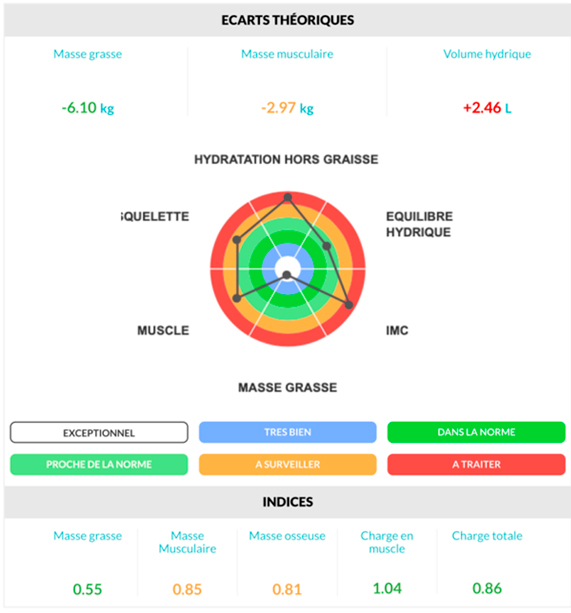
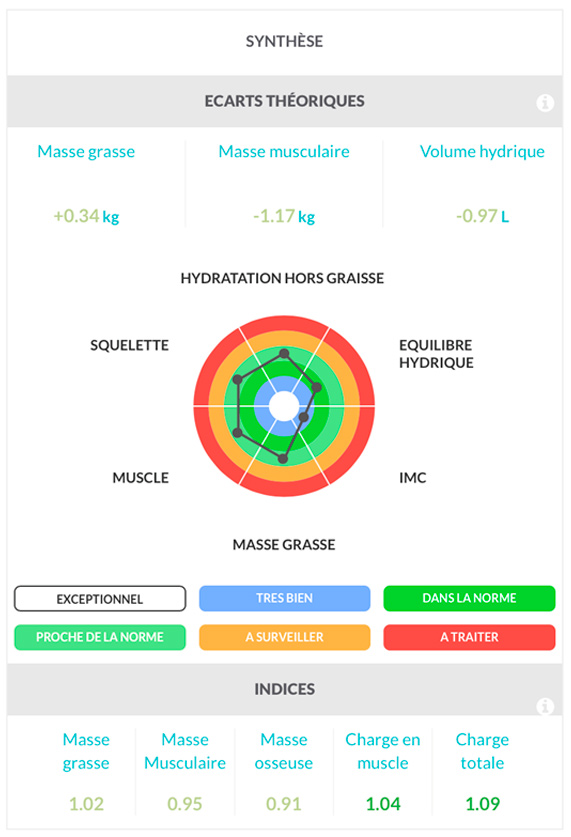
Quick analysis shows that this patient has a slight excess fat mass of 340 g compared to her reference, which is associated with a skeletal muscle mass deficit of 1.17 kg and dehydration of 970 mL. Looking at the indices, we can also observe a 10% bone mass deficit, suggesting that this patient was not in an optimal health state and likely had some silent physiological dysfunctions.

Similarly, considering the patient’s age, height, and weight, the phase angle and impedance ratio values indicate that despite her Covid-19 infection, the patient seems to have normal cellular quality and inflammatory status.
Fat-Free Mass, Total Skeletal Muscle Mass, and Limb Muscle Mass

The compartments most affected by malnutrition are fat-free mass and skeletal muscle mass. Indeed, skeletal muscle is the primary protein reserve in the body, and in a context where protein intake is insufficient, muscle proteins will be degraded to be used by other organs. In this context, two indicators are relevant here: the fat-free mass index (FFMI), recommended by the HAS for the diagnosis of malnutrition¹, and the appendicular skeletal muscle mass index (ASMI), recommended for the diagnosis of sarcopenia⁹. In this patient’s case, we can observe that she has an FFMI and ASMI above the cutoff values, indicating that she does not present malnutrition or sarcopenia at the time of her hospitalization. Despite this, we can notice that both indices are close to the lower limit, indicating that the patient was already in a state of frailty at the time of her admission.
Fat-Free Dry Mass

As mentioned in the previous paragraph, malnutrition is characterized by a loss of protein mass, especially at the muscular level, therefore fat-free dry mass is also a relevant parameter to confirm the onset of malnutrition. At hospitalization, we can observe a slight deficit in proteins and minerals of 420 g, which is consistent with the skeletal muscle mass data and the patient’s morphology.
Fat Mass at Constant Hydration

Since malnutrition can be characterized by a decrease in energy intake, it is also relevant to look at fat mass because lipids constitute the main energy reserve in the body. Cachexia, i.e., malnutrition present in cancer, is particularly characterized by a decrease in fat mass in addition to skeletal muscle mass². In this patient’s case, we can observe that she has a fat mass percentage of 27.69%, close to the health reference.
Quick Analysis – May 2020
| Sex | Female |
| Age | 67 years |
| Height | 165 cm |
| Weight | 54 kg |
| BMI | 19,8 kg/m2 |
| Pathologies | Covid-19 |
| Symptoms | Asthenia, respiratory difficulties, fever, loss of appetite, and changes in taste and smell |
One month after her hospitalization, the patient lost 4 kg of body mass, or 6.9%, and according to the diagnostic criteria recommended by the HAS, this patient is malnourished, which needs to be confirmed with other parameters.

Regarding the phase angle and impedance ratio (IR), we can observe a linear decrease in the phase angle associated with a significant increase in the IR, highlighting a decrease in cellular quality and, therefore, health status, associated with high chronic inflammation. These two events are characteristic of a Covid-19 infection and confirm their importance in monitoring the health status of patients.
Fat-Free Mass, Total Skeletal Muscle Mass, and Limb Muscle Mass

Between the two measurements, the patient presents a loss of 2.7 kg of fat-free mass, 1.92 kg of total skeletal muscle mass, and 1.06 kg of limb skeletal muscle mass. The fat-free mass index (FFMI) value is 14.57 kg/m², which is below the cutoff value of 15 kg/m², indicating that this patient is indeed malnourished. Additionally, the appendicular skeletal muscle mass index (ASMI) is also below the cutoff value of 5.45 kg/m², indicating that this patient is also sarcopenic. Therefore, the body composition values obtained by bioimpedance analysis confirm that this patient’s rapid weight loss is indeed caused by malnutrition.
Fat-Free Dry Mass

The losses of fat-free mass and skeletal muscle mass can be linked to transient dehydration or to the loss of muscle proteins. Since the latter is more detrimental to the body in the long term, it is necessary to monitor the evolution of fat-free dry mass, which corresponds to the total amount of proteins and minerals, to verify that this decrease is indeed related to a loss of protein mass. In this patient’s case, she lost 1.6 kg of fat-free dry mass, confirming that the loss of fat-free mass and skeletal muscle mass are indeed caused by a loss of protein mass. From a physiological perspective, this decrease is explained by the patient’s high pro-inflammatory state, which strongly activates the protein degradation mechanisms within skeletal muscle¹⁰, as well as by the reduction in nutritional intake due to the loss of taste and smell.
Fat Mass at Constant Hydration

In one month, this patient’s fat mass decreased from 16.19 to 15.69 kg, a loss of 500 g; however, her fat mass percentage increased from 27.69% to 27.80%, which seems paradoxical with a decrease in fat mass. This is simply explained by the fact that this percentage depends on weight, and in this patient’s case, her weight loss, and fat-free mass loss, is greater than the fat mass decrease. Therefore, her absolute fat mass represents a larger percentage of her weight, hence the increase. It is important to monitor both the absolute fat mass and fat mass percentage in individuals to accurately characterize their evolution. From a biological perspective, this fat mass loss can be explained by the patient’s decreased appetite, resulting in a lower daily energy intake. Thus, to compensate for this decreased energy intake, the body uses the lipids from fat mass as an energy substrate to maintain its activity over time.
Conclusion
Covid can be responsible for significant malnutrition, like many pathologies characterized by a high pro-inflammatory state. As recommended by the HAS¹, bioimpedance analysis is a tool that allows for the detection and monitoring of malnutrition in at-risk patients. For this purpose, several parameters can be used, including fat-free mass, limb skeletal muscle mass, and fat-free dry mass, which allow for the detection of a decrease in protein mass characteristic of malnutrition.