The 33rd European Congress of Obesity (ECO2026), held in Istanbul from 12–15 May 2026, offered a comprehensive view of the current state and future directions of the obesity field.
The obesity field is at a pivotal moment, shaped by three converging forces: the pharmacological revolution driven by GLP-1/GIP receptor agonists, the push to reframe obesity as a chronic disease, and a growing interest in the neurobiological and genetic underpinnings of appetite and weight regulation. There is also a clear emphasis on the treatment of specific populations, including children and older adults.
Pharmacological revolution and the place of BIA
Obesity Management Medications (OMMs) dominated the clinical agenda. The molecular trajectory moves clearly from GLP-1 monotherapy through dual GLP-1/GIP agonism toward triple and quintuple polyagonists, with the stated premise that more receptor targets deliver greater metabolic benefit. Oral GLP-1 agonists address the access and adherence limitations of injectable therapy. The therapeutic goal has shifted from weight loss per se to systemic cardiometabolic benefit — cardiovascular outcomes, MASH/MASLD, HFpEF, and kidney function all featured. Lean mass preservation remains the central unsolved problem.
Maintenance of weight loss was the most clinically urgent theme. Multiple trials demonstrated that weight returns predictably when effective drugs are stopped, framing long-term or indefinite treatment as the biological necessity. Personalisation, predicting individual response upfront, was also identified as a present challenge. The IFSO-EC session positioned OMMs and bariatric surgery as complementary and sequential rather than competing. Digital care programmes confirmed that trial-level efficacy requires structured real-world delivery to translate.
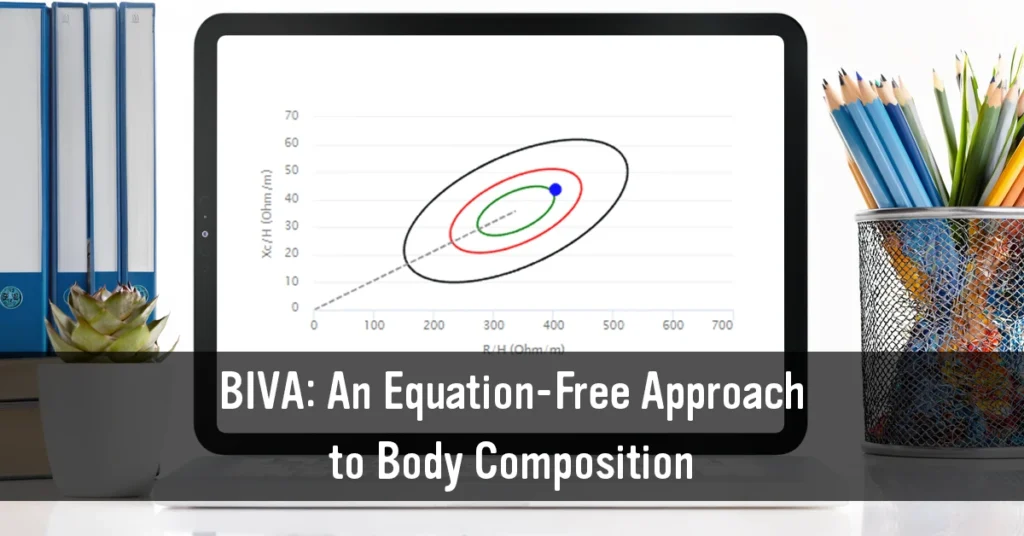
The rapid expansion of obesity pharmacotherapy creates a concrete clinical need that BIA is well positioned to address. Weight on the scale and BMI are insufficient metrics. BIA enables the systematic quantification of fat mass loss, fat-free mass loss, and skeletal muscle preservation over the course of treatment.
Several ECO2026 presentations highlighted lean mass loss as one of the most pressing unresolved issues of the GLP-1 era: a retrospective BIA analysis examined skeletal muscle preservation during GLP-1 receptor agonist therapy (PO4.230)5. Multiple trials for polyagonist molecules report effects on body composition, muscle strength and physical function as primary endpoints, reflecting growing recognition that body composition, not only weight, must be tracked in the new pharmacological era. BIA offers a practical, low-cost tool for longitudinal tracking in real-world clinical settings where DXA is not routinely available.
One of the more scientifically novel directions suggested at ECO2026 concerns BIA spectroscopy parameters that go beyond classical compartmental measurements. A late-breaking poster (LBP4.152)6 presented a pilot study using membrane capacitance obtained by bioimpedance spectroscopy to evaluate insulin resistance. Phase angle was also explored in relation to diabetic peripheral neuropathy (PO4.294)7 and functional parameters in women with obesity (LBP4.143)8. These data suggest that BIA spectroscopy may capture metabolic information that extends beyond body composition per se, potentially providing surrogate markers of metabolic health that could track the effects of complex pharmacological interventions at the cellular level.
Obesity as a chronic disease: positioning BIA in the new diagnostic framework
The central debate, presented in a joint session with the Asian Oceanian Association for the Study of Obesity (AOASO): “Obesity Guidelines — Lancet Commission vs EASO Framework” (Kim, Korea)3, opposed two frameworks: the Lancet Commission (2025)1, distinguishing preclinical from clinical obesity based on organ dysfunction, and the EASO2 staging approach, which applies chronic disease management principles analogous to cardiology. Both move beyond BMI, but with different operational criteria. The shared argument — that BMI is simultaneously over-inclusive and under-inclusive as a diagnostic tool — was also supported by quantitative poster data titled “The WHO BMI classification system inflates the rates of overweight and obesity”.
The Lancet Commission1 explicitly includes direct body fat measurement — by DXA or by bioimpedance — as one of the valid methods for confirming excess adiposity in the diagnostic pathway, alongside anthropometric criteria. This formally positions BIA within the diagnostic algorithm for obesity at an international level for the first time. The COMPARE-DEXA Study, presented in two posters at ECO2026 (PO4.158 and PO4.164)9, directly tested whether BIA can serve as an alternative to BMI for obesity classification, providing empirical grounding for this diagnostic role.
Childhood and adolescent obesity
The paediatric track at ECO2026 balanced therapeutic optimism — the RESETTLE RCT of semaglutide in children, national real-world rollout in Iceland and the UK, and expanding treatment to younger and rarer genetic forms — against evidence-based caution: eating disorder risk (the EDIT Collaboration), the need for wrap-around care, and equity concerns around access.
The paediatric field raises specific challenges for body composition assessment that BIA is in a strong position to address. The Lancet Commission itself acknowledges that body fat percentage and waist circumference do not have clear and generally accepted cut-offs for children — a gap that BIA-based research could help close. At ECO2026, a poster validated bioelectrical impedance equations for predicting fat mass in South African children (PO3.005)10. Critically, as pharmacological treatment of childhood obesity advances the need for accessible, repeatable, and non-invasive body composition monitoring in paediatric clinical practice becomes acute.
Body composition at ECO2026
Body composition featured as a recurrent background variable throughout the congress. Approximately 50 posters included body composition measurements, of which around 25 specified the measurement method in the title. BIA and DXA appeared in comparable numbers, with BIA slightly more frequent; MRI was confined to research and validation contexts; CT to visceral fat quantification and bariatric outcomes; ultrasound to two exploratory posters. A notable sub-theme across several posters concerned muscle and lean mass preservation during GLP-1 therapy — a growing clinical concern, given that these drugs cause substantial loss of fat-free mass alongside fat.
BIA to support patient adherence and engagement
The congress devoted considerable attention to treatment adherence and the patient experience in long-term pharmacotherapy. BIA offers a dimension that weighing scales do not: it makes the metabolic quality of weight loss visible to patients, becoming a potentially powerful motivational and therapeutic communication tool. In the context of programmes designed to optimise adherence to incretin-based therapies (such as the Roczen4 and Oviva digital programmes presented at ECO2026), integrating BIA feedback into patient-facing monitoring could strengthen engagement by concretising and validating the biological changes occurring during treatment.
References
- Rubino F, Cummings D, Eckel R et al., Definition and diagnostic criteria of clinical obesity, The Lancet Diabetes & Endocrinology, 2025; 13, 221-262
- Busetto L, Dicker D, Fruhbeck G, Halford JCG, Sbraccia P, Yumuk V, et al. A new framework for the diagnosis, staging and management of obesity in adults. Nat Med. 2024;30:2395–9. doi: 10.1038/s41591-024-03095-3.
- Cho S, Kwon H. Current guidelines and future directions in comprehensive obesity assessment. Korean J Fam Med. 2026 Jan;47(1):4-11. doi: 10.4082/kjfm.25.0275. Epub 2025 Dec 4. PMID: 41338668; PMCID: PMC12835669.
- Brown A, Dobbie LJ, Falvey L, Patel DC, Kwan JTC, Steinmo S, Chow L, McGowan BM. Real-world data of a digitally enabled, time-restricted eating weight management program in public sector workers living with overweight and obesity in the United Kingdom: A service evaluation of the Roczen program. Obes Sci Pract. 2024 Feb 9;10(1):e730. doi: 10.1002/osp4.730. PMID: 38344678; PMCID: PMC10858326.
- Frohner EI, Itariu BK, Jürets A. Preservation of skeletal muscle mass during GLP-1 receptor agonist therapy in adults with obesity: a retrospective bioimpedance analysis. Poster PO4.230. 33rd European Congress of Obesity (ECO2026); 14 May 2026; Istanbul, Turkey.
- Griene N. Membrane capacitance obtained by bioimpedance spectroscopy to evaluate insulin resistance: a pilot study. Late-Breaking Poster LBP4.152. 33rd European Congress of Obesity (ECO2026); 12–15 May 2026; Istanbul, Turkey.
- Russo B, Menduni M, Coccaro F, Sonnino R, Brunetti M, Simonelli I, Fanali C, Tammaro A, Zanchi G, Silenzi A, Monteleone V, Varì R, Scazzocchio B, D’Archivio M, Frontoni S, Picconi F. Relation between phase angle and diabetic peripheral neuropathy symptoms in patients with metabolic syndrome and type 2 diabetes mellitus: gender differences. Poster PO4.294. 33rd European Congress of Obesity (ECO2026); 14 May 2026; Istanbul, Turkey.
- Sammarco R, Alicante P, Natale R, Morena A, Pagano G, Colasanto S, Scalfi L, Pasanisi F, Marra M. Relationship between segmental phase angle and functional parameters in adult females with obesity. Late-Breaking Poster LBP4.143. 33rd European Congress of Obesity (ECO2026); 12–15 May 2026; Istanbul, Turkey.
- Alotaibi H, Alfraidi A, Altunisi F, Selan J, Almuhaidib S, Alhazzani W. Is bioelectrical impedance an alternative to body mass index for obesity classification? Results from the COMPARE-DEXA Study. Poster PO4.164. 33rd European Congress of Obesity (ECO2026); 14 May 2026; Istanbul, Turkey.