Bioelectrical Impedance Vector Analysis (BIVA) is a non-invasive, equation-free method that evaluates hydration status and soft-tissue body composition using the bivariate analysis of raw electrical data obtained from bioelectrical impedance analysis (BIA).
BIVA’s Evolution: Thirty Years of Progressive Refinement
Since its introduction in 1994 by Piccoli et al.,1 BIVA has evolved from a nephrology-specific monitoring tool into a versatile and clinically useful body composition method available today. Due above all to Piccoli’s foundational work and Campa’s tireless effort to build population-specific reference standards, BIVA has become a globally adopted framework.
The publication of the first tolerance ellipses by Piccoli et al. in 19952 provided the 50th, 75th, and 95th percentile reference regions that clinicians and researchers used for nearly three decades. In 2023, Campa et al.3 conducted a multicentric study of 4,367 healthy adults that replaced those original ellipses with a rigorously updated adult reference. The same group published dedicated reference standards for older adults in 20254 and sport-specific tolerance ellipses for athletes in 20195. In 2025, a comprehensive review by Serafini and colleagues6 mapped all 508 BIVA tolerance ellipses published between 1994 and July 2025, identifying 53 reference studies spanning general adults, children and adolescents, athletes, and pathological populations.
The growing use of BIVA reflects its unique advantages: it requires no predictive equations, is independent of body weight, and is sensitive to fluid shifts. In addition, it provides complementary information on hydration status and body cell mass quality.
BIVA and the Physics Behind the Vector
Using the same principles and measurement techniques as BIA, resistance and reactance are measured and used together to define the impedance vector.
Resistance (R) is the real component of the impedance vector (x-axis) and represents the opposition to electrical current arising from ion-containing body fluids. Lower resistance indicates greater fluid content, whereas higher resistance suggests relative dehydration.
Reactance (Xc) is the imaginary component of the impedance vector (y-axis) and represents the capacitive opposition produced by cell membranes. A high Xc reflects healthy, membrane-rich tissue, as seen in well-trained or well-nourished individuals, whereas a reduced Xc indicates membrane alterations, cell loss, or progressive tissue wasting.
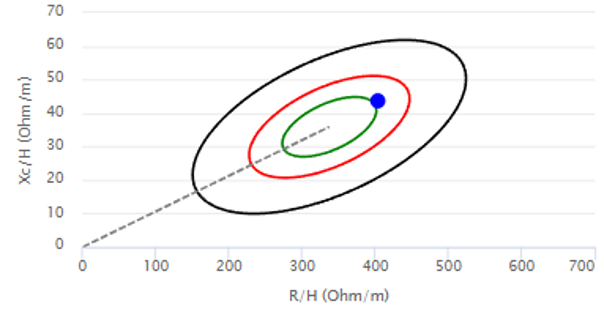
The length of the impedance vector is inversely related to total body water, whereas its direction is related to the phase angle (PhA), a dimensionless marker of cellular health and membrane integrity. To enable valid comparisons among individuals of different statures, both R and Xc are normalized to height (h), yielding R/h and Xc/h expressed in Ω/m (Fig. 1)
BIVA Interpretation: A Short Guide for Clinicians
The individual impedance vector is plotted within the 50th, 75th, and 95th percentile tolerance ellipses of the appropriate reference population. Vector length primarily reflects hydration status: shorter vectors indicate fluid overload or hyperhydration, whereas longer vectors indicate dehydration. Vector direction primarily reflects cellular status: leftward displacement is associated with greater body cell mass, while rightward displacement is associated with reduced body cell mass. The graphical information can be converted into quantitative scalar scores—the HP (Hydration Parameter) and NP (Nutritional Parameter) scores—facilitating longitudinal monitoring, treatment guidance, and outcome assessment.
Clinical nutrition is one of the main applications of BIVA, enabling the identification of oedema, fluid overload or dehydration, and muscle wasting associated with malnutrition, cancer cachexia, and prolonged illness7. Because it is independent of body weight and predictive equations, BIVA is particularly useful in critical care, where it provides a non-invasive bedside tool for monitoring fluid balance and cellular deterioration.
In sports science, BIVA is increasingly used to monitor body cell mass, hydration status, recovery from injury, and the effects of weight cutting in athletes5. Its adoption is growing across professional football, rugby, cycling, and combat sports.
BIVA has also emerged as a valuable tool for assessing sarcopenia and ageing. Reference ellipses developed by Campa and colleagues in 20254 now allow accurate classification of adults aged 65 years and older.
In paediatrics, BIVA has been validated for obesity assessment, malnutrition screening, and sports monitoring6. Reference ellipses are available from four years of age, providing clinicians with a body-weight-independent, equation-free assessment tool.
Future Perspectives and Research Directions in BIVA
BIVA remains a developing field. A key priority is the establishment of ethnically diverse reference standards, as most published tolerance ellipses are derived from European and Latin American populations6. Major ethnic groups, including South and East Asian, Sub-Saharan African, and Middle Eastern populations, remain underrepresented. The BIA International Database initiative (Silva, Campa et al., 2023) is the most systematic effort to address this gap by pooling raw bioelectrical data from populations worldwide.
Multi-frequency BIVA may provide richer information on intra- and extracellular water distribution and tissue electrical properties, potentially improving the detection of early pathological fluid changes and enabling more detailed body composition assessment. Likewise, segmental and localized BIVA could improve spatial resolution, allowing clinicians to identify regional fluid accumulation, asymmetric muscle loss, and injury-related tissue changes that may be overlooked by whole-body measurements.
Perhaps most importantly, integrating BIVA into longitudinal digital health frameworks could fully exploit its greatest strength: repeated-measures monitoring. The ability to non-invasively track hydration status, nutritional status, and cellular integrity over weeks, months, or years—in the hospital, clinic, or field—positions BIVA as a valuable tool for personalized monitoring and precision healthcare.
References
- Piccoli A, Rossi B, Pillon L, Bucciante G. A new method for monitoring body fluid variation by bioimpedance analysis: the RXc graph. Kidney Int. 1994;46(2):534–539. https://doi.org/10.1038/ki.1994.305
- Piccoli A, Nigrelli S, Caberlotto A, et al. Bivariate normal values of the bioelectrical impedance vector in adult and elderly populations. Am J Clin Nutr. 1995;61(2):269–270. https://doi.org/10.1093/ajcn/61.2.269
- Campa F, Coratella G, Cerullo G, et al. New bioelectrical impedance vector references and phase angle centile curves in 4,367 adults: the need for an urgent update after 30 years. Clin Nutr. 2023;42:1749–1758. https://doi.org/10.1016/j.clnu.2023.08.017
- Campa F, Annunziata G, Barrea L, et al. Bioelectrical impedance vector analysis in older adults: reference standards from a cross-sectional study. Front Nutr. 2025;12:1640407. https://doi.org/10.3389/fnut.2025.1640407
- Campa F, Matias C, Gatterer H, et al. Classic bioelectrical impedance vector reference values for assessing body composition in male and female athletes. Int J Environ Res Public Health. 2019;16(24):5066. https://doi.org/10.3390/ijerph16245066
- Serafini S, Mascherini G, Vaquero-Cristóbal R, Esparza-Ros F, Campa F, Izzicupo P. Reference tolerance ellipses in bioelectrical impedance vector analysis across general, pediatric, pathological, and athletic populations: a scoping review. J Funct Morphol Kinesiol. 2025;10(4):415. https://doi.org/10.3390/jfmk10040415
- Piccoli A, Codognotto M, Piasentin P, Naso A. Combined evaluation of nutrition and hydration in dialysis patients with bioelectrical impedance vector analysis (BIVA). Clin Nutr. 2014;33(4):673–677. https://doi.org/10.1016/j.clnu.2013.08.007